Table of Contents
Introduction
Renal Cell Carcinoma (RCC) is the most common type of kidney cancer in adults, comprising about 85–90% of all primary renal malignancies. It arises from the epithelial cells of the proximal renal tubules. RCC is notorious for being asymptomatic in early stages, earning its reputation as a “silent killer.” However, advancements in imaging techniques, molecular diagnostics, and targeted therapy have significantly improved detection and outcomes.
Incidence and Epidemiology
- Renal Cell Carcinoma (RCC) accounts for about 2–3% of all adult cancers globally.
- It is more commonly diagnosed in males than females, with a ratio of approximately 2:1.
- Peak incidence occurs between 60 and 70 years of age.
- The incidence has been increasing worldwide, partly due to widespread use of imaging modalities.
- Higher rates are seen in North America and Europe compared to Asia and Africa.
Risk Factors
- Modifiable Risk Factors:
- Smoking (doubles the risk)
- Obesity (especially in postmenopausal women)
- Hypertension
- Chronic analgesic abuse (especially phenacetin)
- Occupational exposures (cadmium, asbestos, trichloroethylene)
- Non-Modifiable Risk Factors:
- Family history of Renal Cell Carcinoma (RCC)
- Chronic kidney disease and dialysis
- Genetic predisposition (e.g., von Hippel–Lindau disease, Birt–Hogg–Dubé syndrome, HLRCC)
Pathology and Subtypes
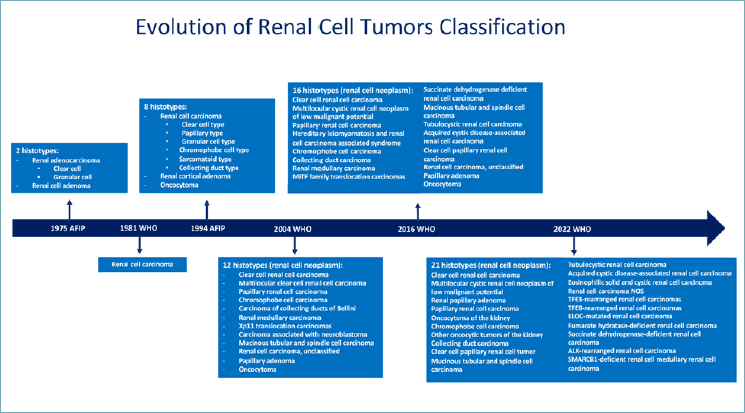
Renal Cell Carcinoma includes several subtypes:
- Clear Cell RCC (ccRCC) – ~75–80%
- Associated with VHL gene mutation
- Characterized by lipid- and glycogen-rich cells
- Papillary RCC (Type 1 and 2) – ~10–15%
- Type 1 is less aggressive; Type 2 has worse prognosis
- Chromophobe RCC – ~5%
- Generally has better prognosis
- Collecting duct carcinoma and Medullary carcinoma – Rare but very aggressive
Clinical Presentation
Often asymptomatic in early stages and detected incidentally. Classical triad (rare):
- Hematuria (gross or microscopic)
- Flank pain
- Palpable abdominal mass
Other signs and symptoms:
- Fatigue
- Weight loss
- Fever without infection
- Varicocele (left-sided due to renal vein obstruction)
- Hypertension
- Polycythemia (due to ectopic erythropoietin)
- Hypercalcemia (due to PTHrP production)
- Metastatic symptoms: bone pain, cough, dyspnea
Diagnosis
- Imaging:
- Ultrasound: Often first test in hematuria workup
- CT abdomen with contrast: Gold standard for diagnosis and staging
- MRI: Preferred in patients with contrast allergy or impaired kidney function
- Chest X-ray or CT thorax: For metastasis evaluation
- Laboratory tests:
- CBC: May show anemia or polycythemia
- Renal function tests
- Liver function tests (Stauffer’s syndrome)
- Serum calcium and LDH
- Urinalysis: May show microscopic hematuria
- Biopsy:
- Not routinely done for resectable masses
- Used in metastatic or unresectable cases to guide systemic therapy
Staging (TNM Classification)
- Stage I: Tumor ≤7 cm, confined to kidney
- Stage II: Tumor >7 cm, still confined to kidney
- Stage III: Spread to major veins or adrenal gland
- Stage IV: Distant metastasis or regional lymph node involvement
Treatment
Localized RCC (Stages I–III)
- Surgical Options:
- Radical nephrectomy: Complete removal of the kidney and surrounding structures
- Partial nephrectomy: Nephron-sparing surgery, preferred for tumors <4 cm or in solitary kidney
- Ablative therapies: Cryoablation or radiofrequency ablation in non-surgical candidates
- Active surveillance: For small tumors (<3 cm) in elderly or comorbid patients
Metastatic RCC (Stage IV)
- Targeted therapy:
- VEGF inhibitors: Sunitinib, axitinib, pazopanib
- mTOR inhibitors: Everolimus, temsirolimus
- Immunotherapy:
- Checkpoint inhibitors: Nivolumab, pembrolizumab, ipilimumab
- Combination regimens: e.g., nivolumab + ipilimumab or pembrolizumab + axitinib
- Cytoreductive nephrectomy: Beneficial in select metastatic cases
- Radiation and palliative care: For bone and brain metastases
Lifestyle and Prevention
- Quit smoking
- Maintain a healthy BMI
- Control blood pressure
- Avoid unnecessary analgesics
- Regular screening for high-risk individuals (genetic predisposition, family history)
Prognosis
- 5-Year Survival Rates (Based on Stage):
- Localized (Stage I): ~93%
- Regional (Stage II–III): ~69%
- Distant metastases (Stage IV): ~13%
- Prognostic factors:
- Stage and grade
- Performance status
- Time to metastasis
- Laboratory markers (calcium, LDH, hemoglobin)
Recent Research and Advancements
- Genomic Profiling: Use of next-generation sequencing to identify targetable mutations
- Newer Immunotherapy Combinations: Dual checkpoint blockade and combinations with TKIs show improved progression-free survival
- Liquid Biopsies: Non-invasive detection and monitoring of circulating tumor DNA
- Artificial Intelligence in Imaging: AI tools to improve early detection and precision in staging
- Neoadjuvant and Adjuvant Therapies: Trials evaluating systemic treatment before and after surgery for better outcomes
Follow-Up and Surveillance
- First 3 years: Imaging every 6 months
- After 3–5 years: Annually, based on recurrence risk
- Monitor renal function, blood pressure, and for signs of recurrence or metastasis
Frequently Asked Questions (FAQs)
1. What are early signs of Renal Cell Carcinoma (RCC) ? Most cases are asymptomatic early. Hematuria or incidental findings on imaging are often the first clues.
2. Is Renal Cell Carcinoma (RCC) curable? Yes, if diagnosed early and localized, it is often curable with surgery.
3. How is RCC different from other kidney cancers? RCC arises from the renal tubules and is more resistant to chemotherapy compared to other types like transitional cell carcinoma.
4. Can kidney cancer spread to other organs? Yes, common sites include lungs, bones, liver, and brain.
5. Does Renal Cell Carcinoma (RCC) run in families? Hereditary forms exist, such as VHL syndrome. Genetic counseling is recommended for those with a strong family history.
6. Can lifestyle changes prevent Renal Cell Carcinoma (RCC) ? Yes. Avoiding smoking, managing weight and blood pressure, and limiting harmful chemical exposures can reduce risk.
7. What is the role of immunotherapy in Renal Cell Carcinoma ? It has revolutionized treatment for metastatic RCC, significantly improving survival in advanced stages.
8. Are there any blood tests to detect RCC? No specific blood test exists for early detection, but labs can help in diagnosis and prognosis.
9. What is the life expectancy after Renal Cell Carcinoma (RCC) diagnosis? Depends on the stage. Localized disease has excellent prognosis; metastatic cases vary widely with treatment response.
10. Is dialysis needed after kidney removal? Not if the remaining kidney functions normally. Dialysis may be needed in those with poor residual function or both kidneys affected.
Conclusion
Renal Cell Carcinoma is a significant health concern with increasing global incidence. Despite being potentially silent in early stages, advancements in imaging, surgical techniques, targeted therapy, and immunotherapy have transformed its management. Continued research and awareness can further improve early detection, personalized treatment, and survival outcomes. Regular follow-up and patient education remain crucial pillars in managing RCC effectively.
For more updates, follow us on X (Twitter), Instagram & Facebook. And our website MED COLLEGE DARSHAN.

No responses yet